Newsletter Subscribe
Enter your email address below and subscribe to our newsletter
Enter your email address below and subscribe to our newsletter

The contemporary landscape of Australian healthcare demands an unprecedented level of agility, critical acumen, and practical readiness from graduate nurses. As the clinical environment grows increasingly complex—characterized by an aging population, multi-morbidities, rapid technological integration, and systemic post-pandemic resource constraints—the academic systems preparing these professionals face intense scrutiny. Central to this discourse is the historic and persistent “theory-practice gap”: the operational disconnect between the conceptual knowledge acquired within university lecture theatres and the chaotic, fast-paced realities of live clinical environments. This text provides an expansive, data-driven examination of how Australian nursing education is actively working to dismantle this barrier, empowering future clinicians to transition seamlessly from the classroom to the acute care ward.
In academic literature, the theory-practice gap is defined not as an absolute failure of education, but rather as an operational dissonance. In the controlled environment of a university simulation laboratory, clinical skills are taught linearly. A student learning to insert a peripheral intravenous cannula or administer an intramuscular injection follows a structured, sequential checklist. The environment is quiet, the manikin is stationary, and time is an open resource. However, upon entering an acute medical ward during a frantic shift handover, that same student encounters immediate cognitive overload. The patient may be delirious, the clinical setting is dynamic, and systemic distractions are omnipresent.
Statistics within the Australian context highlight the operational friction experienced by transitioning students. Longitudinal graduate surveys show that while over 85% of nursing graduates feel theoretically competent upon completing their bachelor’s degrees, less than 48% feel immediately confident in handling acute clinical escalations or navigating complex multi-patient allocations independently. This drop-off in perceived readiness highlights the strategic value of specialized academic intervention. Navigating the transition into tertiary healthcare courses requires an adjustment to advanced university grading rubrics. For many incoming students, utilizing targeted regional assessment help within Australia is a foundational step to mastering academic formatting and passing initial core modules, thereby freeing up valuable cognitive bandwidth for hands-on clinical lab practice.
This operational disconnect is further exacerbated by the varying structures of clinical placement models across Australian jurisdictions. Undergraduate nursing students in Australia are mandated by national registration authorities to complete a minimum of 800 hours of supervised clinical practice throughout their program. However, the pedagogical structure of these hours varies significantly between block placements (where students spend several consecutive weeks in a hospital) and distributed placement models (where clinical days are interspersed with academic study). Each model presents distinct challenges in knowledge retention, skill consolidation, and professional identity development.
To systematically address this operational divide, Australian higher education providers have invested heavily in sophisticated Simulation-Based Learning (SBL). Modern simulation goes far beyond low-fidelity task trainers to encompass high-fidelity human patient simulators (HPS), virtual reality (VR) clinical environments, and standardized patient programs utilizing professional actors.
High-fidelity simulators mimic realistic physiological responses, including pupillary changes, cardiac arrhythmias, abnormal breath sounds, and vocalized complaints. Through structured clinical scenarios, students are forced to apply theoretical knowledge under realistic time constraints. For instance, a scenario involving an acute anaphylactic reaction requires the student to recognize the early clinical signs, calculate correct medication dosages, prioritize interventions, and communicate using frameworks such as ISBAR (Introduction, Situation, Background, Assessment, Recommendation). By experiencing these high-stakes scenarios within a psychologically safe environment, students build the neural pathways necessary to execute these skills under real-world pressure.
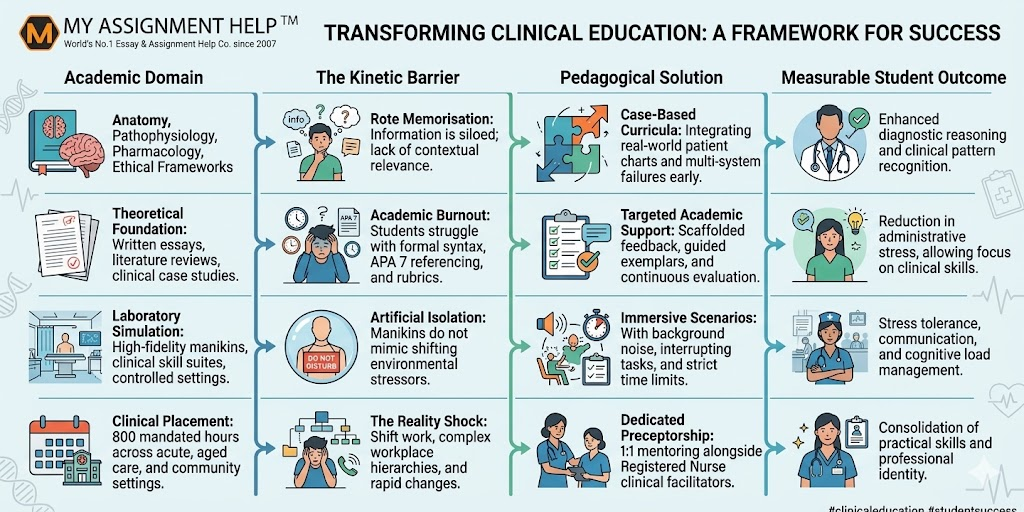
Below is an interactive conceptual blueprint illustrating how modern pedagogy breaks down clinical barriers:
A significant, often underestimated component of the theory-practice gap lies in the realm of clinical communication and formal documentation. Nursing students frequently excel at physical, hands-on tasks, but face substantial hurdles when translating those actions into legally robust documentation. In Australia, documentation must align with strict professional frameworks, including the Nursing and Midwifery Board of Australia (NMBA) Registered Nurse Standards for Practice.
When moving from general science modules into complex patient care plans and evidence-based practice portfolios, the technical requirements skyrocket. Because formatting a flawless clinical case study leaves zero room for error, securing the best nursing assignment help becomes a vital resource for balancing hospital shifts with academic deadlines. Writing an academic analysis of a patient’s hemodynamic instability requires a seamless synthesis of pathophysiology, pharmacological interventions, and nursing rationale. If a student is overwhelmed by the mechanics of literature synthesis or clinical reasoning models, their capacity to perform safely on the clinical floor is heavily compromised.
Moreover, modern clinical documentation in Australian healthcare centers heavily utilizes Electronic Health Records (EHR). Universities are increasingly integrating simulated EHR platforms into their curricula to ensure students are proficient in digital health literacy before their first placement. Understanding how to interpret trend data—such as charting a patient’s deteriorating vital signs using the “Between the Flags” track and trigger system—is critical to preventing adverse patient outcomes.
Evidence-Based Practice (EBP) serves as the primary mechanism for closing the theory-practice gap. EBP demands that clinicians integrate the best available research evidence with clinical expertise and patient values. In the past, nursing interventions were frequently governed by tradition or institutional habit—the “we have always done it this way” mentality. Modern Australian nursing education dismantles this outdated approach by embedding research literacy into every stage of the curriculum.
Students are taught to formulate precise clinical questions using frameworks such as PICO (Population, Intervention, Comparison, Outcome). For example, a student might investigate whether the use of chlorhexidine compared to normal saline for central venous access device (CVAD) dressing changes reduces the incidence of catheter-associated bloodstream infections in intensive care units. By conducting systematic literature searches, critically appraising randomized controlled trials, and translating those findings into clinical care pathways, students actively experience theory transforming into practical, life-saving clinical action.
The translation of theoretical knowledge into clinical practice is nowhere more critical than in clinical calculations. Medication errors represent one of the most significant threats to patient safety globally. In Australian nursing education, students must demonstrate absolute mathematical competence, frequently requiring a 100% pass mark in medication calculation examinations before being permitted to enter clinical placement.
Consider the basic, yet high-stakes, formula used daily by clinicians for calculating intravenous infusion rates:
\text{Infusion Rate (mL/hr)} = \frac{\text{Total Volume (mL)}}{\text{Total Time (hr)}}
For micro-dosing or pediatric applications involving explicit drop factors, the formula expands to account for the administration set’s calibration:
\text{Drip Rate (gtts/min)} = \frac{\text{Volume (mL)} \times \text{Drop Factor (gtts/mL)}}{\text{Time (min)}}
A single decimal error, or a failure to translate a theoretical formula into clinical practice, can result in sub-therapeutic dosing or catastrophic toxicity. This absolute precision highlights why academic rigorousness and technical preparation are foundational to physical bedside safety.
No matter how advanced university laboratories become, the clinical placement remains the ultimate testing ground. To mitigate the “reality shock” that many students experience, Australian healthcare facilities utilize formalized preceptorship and mentorship models. A preceptor is a practicing Registered Nurse (RN) who acts as a one-on-one mentor to the student during their placement, guiding them through clinical workflows, introducing them to organizational cultures, and providing immediate feedback.
Effective preceptorship provides a crucial psychological safety net. It allows the student to progressively take on more complex patient allocations—moving from a single patient to a full workload under direct supervision. Research demonstrates that positive preceptor-student relationships significantly improve clinical competence, boost confidence, and reduce graduate attrition rates. When a student feels supported by their preceptor, they are more likely to ask clarifying questions, critically reflect on their practice, and safely integrate theoretical concepts into their daily care routines.
See also: How Crypto Can Improve Financial Inclusion
Nursing is uniquely dynamic, requiring the simultaneous execution of complex psychomotor skills, advanced interpersonal communication, ethical decision-making, and rapid critical thinking under shifting clinical conditions and strict time constraints.
Many Australian tertiary institutions integrate simulated electronic documentation platforms into their laboratory sessions, allowing students to practice charting vital signs, writing nursing notes, and managing digital fluid balance charts before entering a real clinical placement.
It is a standard patient safety track-and-trigger system used across Australian hospitals. It features color-coded charts that help clinicians rapidly identify deteriorating vital signs and activate appropriate clinical review or rapid response teams.
Medication errors can have catastrophic consequences. A single calculation mistake can lead to a fatal overdose or an underdose, making absolute mathematical proficiency a mandatory requirement for patient safety.
This article was authored by a Senior Academic Content Strategist and Nursing Research Specialist at MyAssignmentServices. With over a decade of experience in designing curriculum support frameworks, specialized nursing portfolios, and data-driven educational content, they help tertiary nursing students across Australia navigate complex academic rubrics, clinical documentation standards, and evidence-based practice portfolios to achieve clinical and professional excellence.